
Just this week there is a report from Newcastle and Glasgow universities explaining that it looks as though 'diabetes can be cured'. Reading more carefully, one realises that the right expression would be that diabetes type 2 can be put into remission. Not for everyone, but for enough people (around half of those with diabetes II) to make a significant difference nationally. Remission means no longer needing medication; the blood sugar levels are low enough for the patient to be outside the zone where the label 'diabetic' applies, but I think we will come to interpret this state as being prone to diabetes and that each person so described must maintain vigilance.
Reading the press reports—I have not yet found the study itself— it is clear that the diet used, the 'soup and shake' diet, is down at 800 calories per day, provided entirely by powdered material to which one adds water. So that's a liquid diet, isn't it? Once something like 15 kg has been lost, the body fat level—especially around the pancreas—is often low enough for it to return to proper function. I have no doubt that there are problems: ones I can think of would include (I) with maintaining the conviction to stick to the diet, (ii) moving back to solid food subsequently (iii) maintenance of the weight loss, particularly preventing subsequent weight gain. All three of these imply to me a serious need for support, of the sort that the NHS has increasingly been unable to provide.
The numbers affected? Well, [1] says more than 250,000 people who were on the cusp of developing type 2 diabetes have been referred to classes which offer advice and support on food, diet and exercise.
To this good news we can add that the signs of diabetes type 2 are detectable long before the usual level of diagnosis, so we could quite easily do screening in a preventative way. Essay 190 describes the huge sums we spend in treating diabetes and the consequences (£8.8 billion per year in 2012, 22,000 early deaths). That figure has also been expressed as 10% of the annual budget, but there was a range of numbers describing the total cost, from the 8.8 given to 24 billion. That higher figure is more than the cost of housing support, I think, though I may not have matched up the years correctly. 1 The apparent saving available would allow the NHS to move from care to prevention, something which we need to have happen — without, it would appear, needing to increase the budget for the NHS in any significant way. Good news at many levels, then. We know that diabetes is preventable (more precisely, many cases of what is identified as diabetes need not have happened); what we have been previously told is that, once you have it, you're stuck with it and at best you might 'manage' the condition. This breakthrough suggests that we can do a good deal better than that.
Picking through the report via [2], everyone in the study was obese or overweight, and everyone stuck to the diet for 3-5 months, most lasting to 16 weeks.
After the liquid phase, there was a structured reintroduction of regular food for some meals, then ongoing education and support about how to maintain the lower weight. Diabetes remission, defined as a haemoglobin A1C of less than 6.5%, was achieved in 46% of those who were on the diet (68 patients).1 Only 6 people (4%), of those in the control care group, had remission. At 12 months, nearly one-fourth of those in the diet group had lost 33 pounds or more. No-one in the comparison group lost as much as a kilo.
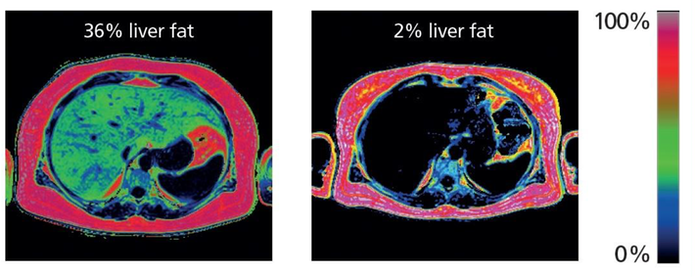
"What happens is the two main abnormalities of type 2 diabetes are both sorted out when weight loss occurs," Dr. Taylor says. "These two abnormalities are brought about by too much fat inside the liver cells and too much fat inside the insulin-secreting cells in the pancreas." [....] While the study participants had all been diagnosed with type 2 diabetes within the past six years, Dr. Taylor says that those diagnosed within the past four years who go on this type of extreme diet have a very good chance of reversing diabetes.
One of the good points about this approach is that it doesn't demand the attendance of an endocrinologist and could be supervised by much less expensive and more available practitioners. The problem is that far too many patients subsequently regain their weight and, if that occurs, then the diabetes returns too. Which says very little about mental stamina, about ability to change habits and about recognition of the need to be free of such a disease. So perhaps it is addressing that part of the problem, that is where the effort needs to move to. Indeed my paltry efforts at exploring this suggest that the British regime is having a lot more success than the US equivalent process, in the sense that many more people are succeeding in keeping their weight down.
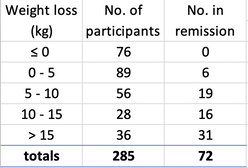
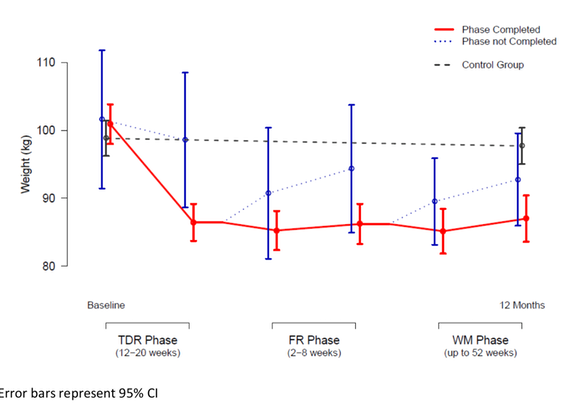
The report itself, possibly linked at [5], indicates a strong correlation between keeping the weight off and staying in remission. Remission varied with weight loss in the whole study population, (DJS' table here). Mean bodyweight fell by 10·0 kg (SD 8·0) in the intervention group and 1·0 kg (3·7) in the control group (adjusted difference −8·8 kg, 95% CI −10·3 to −7·3; p<0·0001). Quality of life, as measured by the EuroQol 5 Dimensions visual analogue scale, improved by 7·2 points (SD 21·3) in the intervention group, and decreased by 2·9 points (15·5) in the control group (adjusted difference 6·4 points, 95% CI 2·5–10·3; p=0·0012). Nine serious adverse events were reported by seven (4%) of 157 participants in the intervention group and two were reported by two (1%) participants in the control group. Two serious adverse events (biliary colic and abdominal pain), occurring in the same participant, were deemed potentially related to the intervention. No serious adverse events led to withdrawal from the study.
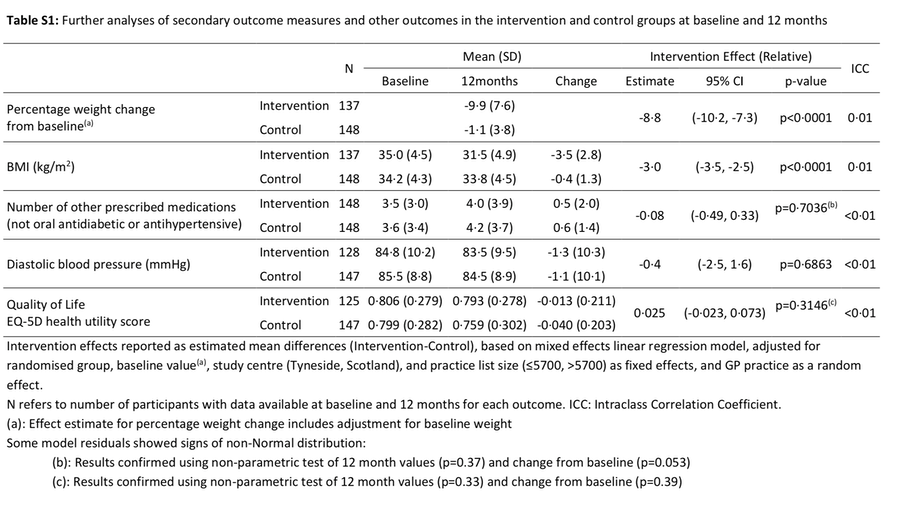
Do try to read the report. If I was still in teaching, I'd take the tables from the appendix and see if I could get an A-level class to understand the statements in the statistical tables, but I think I would need to recreate the original data to cause understanding, which is a pity, since it demonstrates that even the mathematically able would not have a decent grasp of what the statistics are purporting to report, which is at heart a failure to communicate. Perhaps it is worth the work: a matter that affects a significant portion of the population has an approach that might indirectly affect most of us and even the bright end of the population with what would appear to be the necessary understanding cannot grasp the essentials from the given statistics. That seems to me to be a failure, but it fuels the argument that medics might as well study mechanics at school, since the amount of statistics they'll need to absorb in their medical studies is way beyond school, whereas the mechanics (or other alternative such as decision theory) is probably sufficient forever.
DJS 20190308
Top pic from [4] is an MRI scan of the liver, showing high levels of fat in green (left) and a big decrease in fat after a low-calorie diet (right)
[1] https://www.bbc.co.uk/news/health-46363869
[3] https://www.springer.com/us/book/9783319956534 points to the first book on bariatric endocrinology.
[5] https://www.ncl.ac.uk/magres/research/diabetes/reversal/#publicinformation points to the paper itself at the bottom of the page; I've attempted to copy the links here: DiRECT Appendix, (the diagrams) DiRECT Results (the writing)
1 Housing benefit spending as explained by the Office for Budget Responsibility; In our latest forecast, overall outturn spending on housing benefit was estimated to be £21.9 billion in 2017-18, with around £0.8 billion of working-age spending having been ‘lost’ to UC. We expect overall housing benefit spending in 2018-19 to total £23.4 billion, with 4.6 million recipients paid an average of £5,035 each. That would represent 2.9 per cent of total public spending and 1.1 per cent of national income.
Compare this with the info on this site, which is suggesting £14 billion per year of the NHS budget is directly attributable to diabetes and its consequences.
So the £ 24 billion I found (as a sum representing the spend on diabetes and its consequences) in the range of research while writing essay 190 DOES roughly equate to the housing benefit budget.
Previous essays on this topic were 190, Diabetes 2 and 176, Diabetes. They give the numbers of people affected and the trends experienced when I wrote those pieces, with a small amount of subsequent updating.